If you've been asking how complex PTSD differs from PTSD and how it is treated, you are not alone, and the answer matters more than most people realise. Complex PTSD (C-PTSD), despite affecting a significant proportion of people who seek trauma treatment, remains widely misunderstood, including by some mental health practitioners. The two conditions share overlapping symptoms and are both rooted in traumatic experience. The difference lies in what kind of trauma caused them, how deeply that trauma has shaped a person's sense of self, and what it actually takes to heal.
The formal recognition of complex PTSD as a distinct diagnosis in the ICD-11 (the World Health Organisation's International Classification of Diseases, 11th edition) marked a turning point. It validated what trauma specialists had observed for years: that apparent treatment non-response may, in some cases, reflect a missed or incorrect diagnosis rather than the limits of what is possible for that person. At New Paradigm, a specialist residential retreat that works exclusively with complex trauma presentations, this distinction is not an academic detail. It shapes every assessment, every treatment plan, and every decision about how care is structured from day one.
This article covers how complex PTSD differs from PTSD, the evidence-based treatments that work for each condition, the typical care pathway, and practical next steps for Australians seeking specialist support.
What causes PTSD versus complex PTSD
Single traumatic events and how PTSD develops
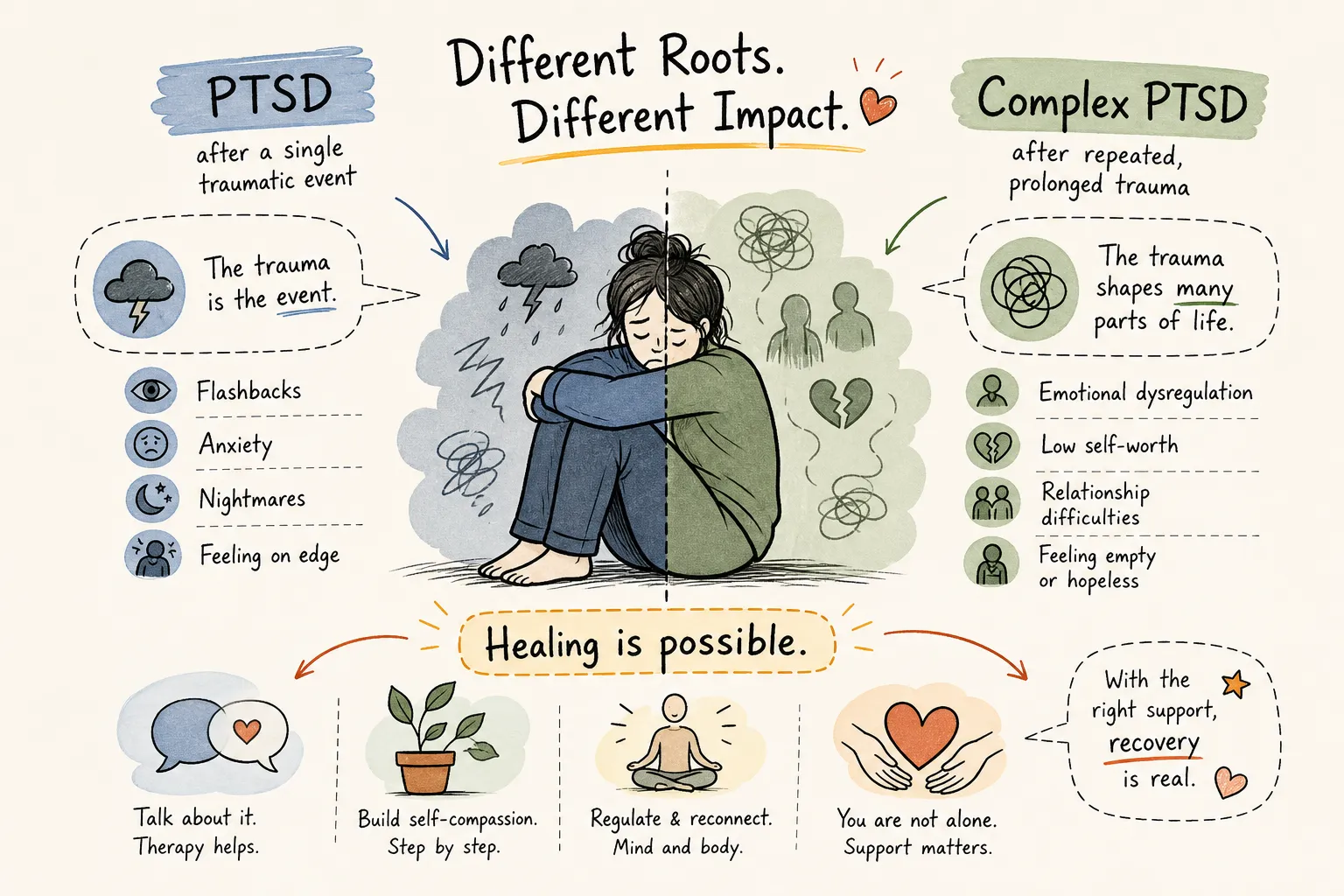
PTSD typically follows a discrete, identifiable event: a car accident, a physical assault, a natural disaster, or a medical emergency. The nervous system becomes conditioned to threat around a specific memory, producing the characteristic symptom clusters of re-experiencing, avoidance, and hyperarousal. Because the trauma has a clear beginning and end, focused trauma-targeted therapy can often achieve meaningful resolution within a manageable timeframe.
Prolonged or interpersonal trauma and the roots of C-PTSD
C-PTSD develops from repeated, inescapable trauma: childhood abuse or neglect, domestic violence, trafficking, or prolonged captivity. The defining factor is entrapment. The person could not leave the source of harm, often because that source was a caregiver or intimate partner. When this trauma begins in early life, it does not simply create frightening memories. It shapes the architecture of attachment, identity, and emotional regulation from the ground up, which is precisely why how complex PTSD differs from PTSD is so evident in clinical presentation.
How is complex PTSD different from PTSD: the symptom profiles
The three core PTSD symptom clusters
ICD-11 defines PTSD through three symptom clusters. Re-experiencing involves intrusive memories, flashbacks, and nightmares in which the event feels present again. Avoidance means steering clear of people, places, thoughts, or feelings connected to the trauma. A persistent sense of current threat manifests as hypervigilance, an exaggerated startle response, and irritability. These symptoms are genuinely impairing, but they remain anchored to a specific event.
The additional disturbances that define complex PTSD
ICD-11 requires all three PTSD criteria to be met for a C-PTSD diagnosis, plus three additional clusters known as disturbances in self-organisation (DSO). Emotional dysregulation involves extreme difficulty managing emotions, from volatile outbursts to complete emotional numbness. A negative self-concept means deep, pervasive shame and a core belief that one is worthless or permanently damaged, qualitatively different from low self-esteem. Relational difficulties describe chronic trouble forming or sustaining close relationships, persistent distrust, and isolation even when connection is desperately wanted.
DSM-5, used more widely in some clinical settings, does not list C-PTSD as a separate diagnosis. Symptoms like shame, guilt, and negative self-view are embedded within an expanded PTSD framework rather than forming a distinct condition. This means that without an ICD-11-informed assessment, C-PTSD can be missed entirely.
Comorbidities and why C-PTSD is so often misread
Common conditions that co-occur with complex PTSD
C-PTSD carries high rates of comorbidity with major depressive disorder, generalised anxiety, insomnia, and borderline personality disorder. Research indicates that approximately 62% of people with C-PTSD experience suicidal ideation, with self-harm and attempt rates also significantly elevated compared with PTSD alone. These figures are not cited to alarm but because they carry direct clinical implications: they affect how treatment must be sequenced and how much support is required throughout the process.
What happens when the wrong model is applied
Because C-PTSD involves identity disturbance and relational problems, it is frequently misdiagnosed as borderline personality disorder, treatment-resistant depression, or generalised anxiety. Some clinical guidelines recommend a stabilisation phase before trauma processing for C-PTSD presentations, with the rationale that moving directly into trauma-focused work without adequate emotional regulation capacity may increase distress or dropout for some clients. Many people with C-PTSD spend extended periods in weekly therapy that addresses symptoms at the surface without reaching the underlying structure of what happened. This is demoralising, and it can entrench the belief that recovery is simply not possible. Correct diagnosis is the first and most consequential step toward a treatment plan that actually fits the condition.
Evidence-based treatments for PTSD and complex PTSD
EMDR and trauma-focused CBT: the frontline treatments
Both EMDR (Eye Movement Desensitisation and Reprocessing) and trauma-focused CBT, including cognitive processing therapy and prolonged exposure, have strong, well-replicated evidence bases for PTSD, supported by major systematic reviews and international clinical guidelines including those published by NICE and Phoenix Australia. For C-PTSD, both remain effective but require considerably more preparation. In EMDR specifically, the stabilisation and resourcing phase is extended to ensure the client can remain emotionally regulated during trauma processing. CBT for C-PTSD explicitly targets the negative self-concept and interpersonal patterns that standard PTSD protocols do not address.
Phased treatment and somatic approaches for complex trauma
Clinical guidelines recommend a phased approach for C-PTSD. Phase 1 focuses on safety, therapeutic alliance, and emotion regulation. Phase 2 addresses trauma processing directly. Phase 3 supports reintegration into a life no longer governed by the trauma. Skills-based interventions such as STAIR (Skills Training in Affective and Interpersonal Regulation) are often integrated in Phase 1 to build the capacity for the processing work that follows.
Somatic therapy works at the body level, addressing the physiological dysregulation that verbal therapies alone cannot fully reach in complex trauma presentations. Techniques such as grounding, pendulation, breath work, and titrated movement (carefully paced physical activity) help the nervous system complete the responses that were thwarted during the original trauma. The research base on somatic approaches is still developing: published randomised controlled trials have shown promising effect sizes for symptom reduction in PTSD and depression, though remission rates vary across studies. The critical clinical point is this: phased C-PTSD treatment requires time, consistency, and a therapeutic relationship built on genuine safety, factors that once-a-week sessions can find difficult to sustain at the pace the condition demands.
How complex PTSD is treated in intensive residential care
The limitations of standard outpatient care for complex trauma
Weekly one-hour sessions offer limited bandwidth for the careful, layered work that C-PTSD requires. Between sessions, clients spend the remainder of the week processing, dysregulating, and waiting with no clinical support available. Building the therapeutic alliance that C-PTSD treatment depends on happens far more slowly in this format. For people with strong emotional dysregulation or high dissociation risk, daily clinical contact is not a luxury. It is a clinical necessity.
What a specialist residential programme offers that outpatient care cannot
In a residential setting, every element of the day, meals, rest, movement, creative work, and daily therapy sessions, can be structured entirely around the client's treatment plan. New Paradigm is a small specialist retreat in Chiang Mai that accepts a maximum of four clients at any one time. One-to-one EMDR, CBT, and somatic work is delivered daily within a low-ratio, highly individualised clinical structure. For Australians who have tried multiple therapists and medications without lasting change, an immersive intensive programme may offer a meaningful step forward, not a reflection on the quality of previous therapists, but on the mismatch between format and clinical need. If you want to read more about residential care specifically, see our definitive guide to residential trauma treatment.
Practical next steps for getting support in Australia
Referral pathways and specialist resources available in Australia
Several well-established pathways exist for Australians seeking specialist trauma support. Blue Knot Foundation is Australia's National Centre of Excellence for Complex Trauma, offering direct phone counselling for survivors, professional training, and evidence-informed resources. Their helpline operates Monday to Sunday (9am, 5pm AEDT) and can be reached on 1300 657 380. Healthdirect (1800 585 585) connects Australians to local mental health services and can help identify trauma-specialist practitioners in their area. Phoenix Australia, the national centre of excellence in posttraumatic mental health, publishes the authoritative Australian clinical guidelines for PTSD and C-PTSD and maintains a practitioner directory. For immediate crisis support, Lifeline is available 24 hours on 13 11 14.
When to consider stepping up to intensive or residential treatment
If you or someone you care for has been in therapy for C-PTSD without meaningful progress, it is worth asking whether the format of care, not the effort, is the limiting factor. Assessment by a trauma-specialist psychologist or psychiatrist using the International Trauma Questionnaire (ITQ), a validated ICD-11 screening tool, can help confirm a C-PTSD diagnosis and guide the appropriate level of care. For more on clinical assessment and essentials for complex PTSD, see this complex PTSD assessment guide. For those who have exhausted standard pathways, a confidential evaluation with a specialist residential programme is a practical, low-commitment next step before making any larger decision. The Blue Knot Foundation helpline is also a useful first port of call for anyone unsure where to begin.
The distinction matters more than most people realise
Understanding how complex PTSD differs from PTSD, and how it is treated differently, is one of the most important steps toward finding care that actually fits. C-PTSD is not a more severe version of PTSD. It is a different clinical picture that developed in different circumstances and requires a different therapeutic approach.
C-PTSD is treatable. With the right modalities, the right format of care, and enough time for the nervous system to genuinely reorganise, real and lasting recovery is possible. What so many people have not yet had is access to care that matches the depth of what happened to them.
If years of weekly therapy have not delivered the freedom you expected, that is not evidence of a personal failing. It may simply mean that the model has not yet matched the condition. Reaching out to the Blue Knot Foundation or requesting a specialist assessment is a concrete first step toward finding out what will.